Just this month an article was published in the Journal of the American Medical Association which assessed the familial risk of autism. This was a gigantic population based study on Swedish children born between 1982 and 2006, which looked at trends in autism spectrum diagnosis amongst monozygotic (identical) and dizygotic (fraternal) twins, full siblings, half siblings, and cousins. Groups were broken down into multiplex (autism occurs more than once) and simplex (only a single child with the diagnosis), so as to look at differences in heritability.
They found that simplex cases of autism, whether twins, full siblings, half siblings, or cousins, ranged from 27-94 cases per 100,000 people per year, which is a fairly small spread, indicating little in the way of heritability (unsurprisingly). On the other hand, monozygotic twins concordant for autism occurred in approximately 6,274 cases per 100,000 people per year, calculated as 59.2% heritability. Meanwhile, dizygotic twins and full siblings exhibited equal rates of heritability, at 12.9% each. Maternally-related half siblings exhibited 8.6% heritability, paternally-related half siblings 6.8%, and cousins 2.6%. In short, the team concluded that, though autism was highly heritable, it was still about 50/50 genes vs. environment, and particularly postnatal environment, since dizygotic twins showed no differences in rates of heritability as compared to full siblings.
What I find absolutely intriguing is that if one looks at these percentages, particularly those of the dizygotic twins/full siblings vs. half siblings vs. cousins, these figures decline by 1/3rd or ~5% across these groupings (see graph below).
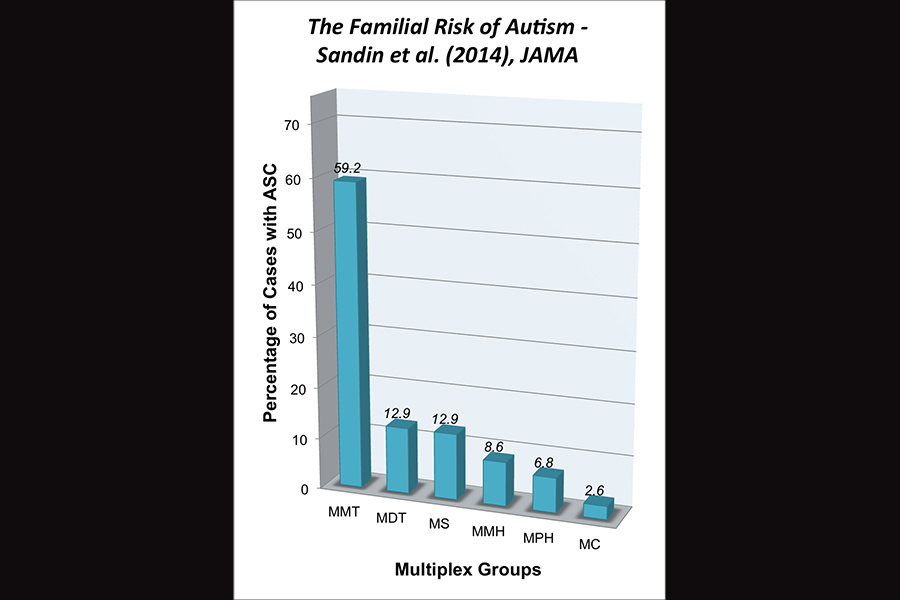
A graph based off the data reported by Sandin et al. (2014) on multiplex families. MMT = multiplex monozygotic twins, MDT = multiplex dizygotic twins, MMH = multiplex maternal half siblings, MPH = multiplex paternal half siblings, MC = multiplex cousins.
Maybe because we know autism in multiplex families is supposed to be heritable, this means that the idea of decreasing heritability the further we get in relatedness is a minor no-brainer. On the other hand, what it suggests to me is that there are discrete units of heritability that are either being inherited or not inherited which ultimately promote autism, with increasing probability the closer one comes to monozygotic twins. Therefore, to me, there’s no no-brainer about it.
Inherited genes are one type of discrete unit with which we’re all familiar and could well explain what were seeing here. However, I just want to remind the reader that genetic inheritance is not the only type of discrete unit of inheritance and that information can lie above the gene (epigenetics) and be inherited as well, though these processes are far less well understood at present.
Finally, this study offers estimates as far as prevalence of simplex versus multiplex cases. It suggests that in Sweden, and probably around the world, simplex cases are comparatively rare, meanwhile cases of autism which have an inherited component are in the large majority. This is a really important point to make, because it can help to pinpoint our research endeavors. Ultimately, we are probably looking for a combination of inherited and environmental triggers, both of which will likely vary by case.
This was an excellent, thorough, and well-designed epidemiological study on the incidence of autism spectrum conditions in a large population study. If you get a chance, I highly recommend a look at the original article by Sandin et al.

Permission to reblog?
Please feel free, Rachellie!
Classical twin studies have never told the true story of inheritance. Down syndrome (1-750) and Klinefelter syndrome (1-500 newborn males) are the most common genetic syndromes associated with high risk of co-occurring autism. Twin studies have found that virtually all monozygotic twins diagnosed with these genetic syndromes are concordant for and virtually all dizygotic twins are discordant for the genetic diagnosis. They are caused by a reproductive error (sperm or egg mutations) and the gene mutation is almost never present in either parent. A tiny percentage is known to have a mosaic condition in which some the cells of a parent have the mutation and some don’t. That is the only cases where ‘inheritance’ is possible. Mosaic Down syndrome and Mosaic Klinefelter syndrome are also not ‘inherited’. Classical twin study design would calculate both of these genetic syndromes as the most ‘heritable’ of all the developmental disorders.
I have argued that strictly defined autism is multifactorial and involves multiple risk factors of small effect that cumulatively increases total risk in any individual case. The question is what exactly is ‘inherited’ in strictly defined autism? I have argued that what is ‘inherited’ in strictly defined autism is not autism but what has come to be called the broader autism phenotype (BAP) or ‘autistic-like traits’ that are traits that are common and widely distributed throughout the general population. The distribution of the BAP in the general population has widely ranged from 5% to 20%. When there is a disruption of early brain development, these mild BAP traits are manifested at the extremes especially in early childhood. Where the familial BAP is not present the outcomes are a variety of debilitating disorders but without co-occurring strictly defined autism.
For further information see:
http://www.ncbi.nlm.nih.gov/pubmed/11079353
Click to access 1379116999.pdf
In terms of the inheritance of BAP, Robert, I’m inclined to heartily agree with you. As you pointed out in previous comments, I believe on the topic of schizophrenia, would be to include families and to better understand BAP and therefore autism in general. As always, thanks for the input. 🙂
It was still about 50/50 genes vs. environment, and particularly postnatal environment, since dizygotic twins showed no differences in rates of heritability as compared to full siblings.
*Start wild speculation*
What is driving me crazy about these results in the increased step from monozyogtic twins to everything else. If these twins share 50% of their genes with brothers/sisters, why is their increase in risk so substantially higher? What environmental components could be attributing to this?
There was an idea being proposed by one resident of the autism-net in particular that the placental status could be a mitigating factor; either a shared placenta or different placentas, with the idea that this could be an input. If I understand correctly (?), this type of relationship was *hoped* to be part of the analysis on a California twin study that had largely similar results (larger environmental input than expected). [http://www.ncbi.nlm.nih.gov/pubmed/21727249] It doesn’t look like that data was included, perhaps insufficient sample size of the chorion type was available. (?) [I bet RAJ knows more on this.]
As a Some-Jerk-On-The-Internet-Armchair-Thinker-Out-Loud, the idea of a shared placenta being a risk factor in off itself could provide an explanation for the disconnect between monozygotic twins and dizygotic twins. Monozygotic twins share a placenta roughly 75% of the time (ala Wikipedia). *If* sharing a placenta is capable of imparting a risk of developing autism (a big if!) this might help explain why there seemed to be such a large jump in risk for monzygotic (and thus, more likely shared placenta) twins compared to dizyogtic and full siblings; they are developing from the first days of being an embryo within an environment that is a risk factor. This would be a pretty nasty revelation considering the dollars and researcher time thrown at genetic analysis on the basis of twin studies defining the (presumed genetic) heritability of autism.
*End wild speculation*
Nice article!
LOL. There’s RAJ, he piped in between the time I loaded the page and got a response typed up. Nicely done!
LOL. As far as sharing a placenta is concerned you make valuable points. Aside from monozygotic twins who share the same de novo gene mutation (Down syndrome), a number of studies have reported that 60% of monozygotic twins are concordant for autism. The 1995 twin study by Rutter’s group reported a 60% concordance rate for strict autism. That is the most referenced autism paper published in the last ten years.
http://www.ncbi.nlm.nih.gov/pubmed/7792363
Not all MZ twins share the same prenatal environment. 2.3rds of MZ twins share the same prenatal environment developing in the same placenta (monochorianic), however 1/3rd of MZ twins do not share the same prenatal environment and develop in seperate placentas just like dyzogotic twins (dichorionic).
http://www.ncbi.nlm.nih.gov/pubmed/7481567
‘The results indicate that concordant MZ pairs were more likely to have been monochorionic (MC) and to have shared a single placenta, whereas discordant MZ pairs appear more likely to have been dichorionic (DC) with separate placentas’
The 60% conundrum that hasn’t been explained or studied much. I was also disappointed that the CATS studies did not include concordance for autism of MZ pairs by chorion type.
Reblogged this on My Puzzling Piece: A Glance Into A Puzzling Existance and commented:
Genetics and Autism: a great study published by the Journal of the American Medical Association. Thank you Emily, from Science Over a Cuppa!
I’m enjoying and learning from the convo; keep going, guys. 🙂
I could go on and on when it comes to twin studies Emily.. A great deal of research has gone into the phenomena of the high male:female (4:1) ratio in autism. Another growing area of interest is the role of skewed X-inactivation found primarily in females. Almost all Rett Syndrome girls have been shown to have skewed X-inactivation patterns. Trejo et al studied 41 MZ twin pairs. 26 with autoimmune disease and 15 newborn females. They found a strong correlation between dichorionic fetal anatomy and differences in X chromosome inactivation patterns between members of an MZ twin pair. In contrast, all monochorionic twin pairs had closely correlated patterns of X chromosome inactivation. Highly similar patterns of X chromosome inactivation among monochorionic twin pairs may result from their shared placental blood supply during intrauterine life. An interesting study that deserves follow-up in autism research particularly what role, if any, skewed X-inactivation may play in autism in females and/or how X-inacivation is expressed in some females meeting strict autism criteria.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2229926/
http://www.nature.com/ejhg/journal/v14/n11/abs/5201682a.html
Robert, do you have a good review or book chapter you could recommend on what is known about the differences in early development between mono- and dichorionic and how the two arise? I.e., what are the causes of mono vs. di.
I don’t know of any chapter on twinning in autism. If there are good chapters they most likely are found in textbooks from Obstetrics and Gynecology. Perhaps someone in the University of Louisville medical center could give you a heads up. Chorionicity and amnionicity of monozygotic gestations are determined by the time at which division of the fertilized ovum occurs. If twinning occurs during the first 2 to 3 days, it precedes the separation of cells that eventually become the chorion and results in a dichorionic diamniotic pregnancy. After approximately 3 days, twinning cannot split the chorionic cavity, and division of an ovum results in monochorionic placentation. The causes of the timing of twinning I don’t think is known.
Sir Francis Galton over 150 years ago was the father of classical twin studies. His method was the precursor of behavioral genetics which relies heavily on twin studies. In his twin research he developed a model which could predict a’ heritability’ estimate by calculating the difference between concordances for any trait in MZ twins compared to DZ twins. Every paper in autism research has used Dalton’s classical twin study design. This method does not distinguish ‘genetic’ from ‘heritability’ and the behavioral geneticists use these terms interchangeably and consider the environment as a nuisance best ignored.
One of the problems was poor obstetrical records prior to the 1970’s or 1980’s. A number of studies found that dichorionic MZ twins were often misdiagnosed as DZ twins. Obstetrical records are now comprehensive in the western democracies especially the Scandinavian countries where all of the best twin studies originate.
I do think that in the future twin studies will become much more comprehensive and include chorion data but that day is not here yet.
Here is the best European twin register (The East Flanders Prospective Twin Survey (Belgium): a population-based register) that so far is nonexistent in the US. The data is there the researchers just have included it in their autism twin studies.
http://www.ncbi.nlm.nih.gov/pubmed/12537855
Thanks, Robert. I managed to find a book along those lines and just ordered it:
Maternal, Fetal, & Neonatal Physiology:
I hear and agree with your frustration about “genetic” versus “inherited”. It’s a tradition of language and concept usage that needs to be ratified in the biological sciences and even everyday conversation. The above study likewise misused the term “genetic” when they should have simply said “inherited”. It’s funny how in the zygote, dormant maternal RNA is inherited which sets the fertilized egg on its trajectory. Once fertilized, those RNAs are finally translated and polarity within the cell starts to occur. I suppose in some way this is “genetic” in the sense that it’s the mother’s genes, but certainly not those of the zygote. And likewise the point of sperm entry helps to determine polarity too.
Thanks for info on the Belgium twin register. That might come in handy some day!
A final observation on the interchangeability of the terms ‘genetic’ and ‘inherited’. A great deal of research is in the field of parental imprinting in genetic disorders with high risk for co-occurring autism. Arthur L. Beaudet is perhaps the world’s leading expert in Prader-Willi and Angelman syndrome. Advances in technology permits identification of the parent of origin for the PW or AS gene mutation. It is often described by behavioral geneticists as being ‘inherited’ from the father or mother. In fact, neither father or mother possess the mutation, the mutation is confined to reproductive cells, sperm or egg mutations.
Here is an excerpt from Dr. Beaudet’s Allan Award lecture:
‘We now know that most cases of Prader-Willi syndrome are caused by paternal deletions of 15q11-q13 and that most cases of Angelman syndrome are caused by maternal deletions of the same region. Now, some years later, it is perfectly obvious that deletion is a genetic form of PWS or AS while UPD is an epigenetic form of PWS or AS. If you could sequence the genome of a UPD patient, it would be normal and give no clue to the source of the phenotypic defect except the possibility of complete lack of heterozygosity at the nucleotide level for part or all of the chromosome. In terms of potential lessons for other disorders, it should be noted that almost all of these genetic and epigenetic cases of PWS and AS are de novo as contrasted to being inherited events. Over the years I have grown to emphasize this distinction with a genetic disease being an aberration of nucleotide sequence causing a disease phenotype in contrast to an epigenetic disease, which can be defined as an aberration in epigenotype (stable/heritable change in gene expression) causing a disease phenotype in the absence of nucleotide sequence aberration. Both can lead to the same biochemical and phenotypic result through altered expression of the same genes’.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2427262/
Hi Emily + RAJ –
I had a few more ideas rattling around my head that I thought I’d throw out there as WAGs on why we might see such a big difference between MZ twins and the rest of the population.
1) Could the process of cleavage in an of itself be a risk factor for generating genetic deletions/duplications/other mixups in the zygotes?
2) Could a maternal environmental or genetic input be a risk factor for cleavage into MZ twins and ASD? It might be interesting to look for ASD rates in some of the twin ‘hotspots’, i.e., Linha São Pedro, which according to one study has a twin birthing rate at 10% (!!!!) [http://www.ncbi.nlm.nih.gov/pubmed/9181177]
3) Regarding the shared placenta environment line of reasoning, there are some studies indicating placenta differences in ASD vs control, including one hot off the presses from IMFAR 2014!
https://imfar.confex.com/imfar/2014/webprogram/Paper16579.html
http://www.ncbi.nlm.nih.gov/pubmed/16806106
http://www.ncbi.nlm.nih.gov/pubmed/23623455
I don’t believe that our knowledge set on shared chorion details are fine grained enough to tell us more, or my Google-Fu is insufficient to uncover it. Maybe the ordered textbook know more. @Emily – Give us an update when you get a chance!
That’s a good distinction, Robert, avoiding the issue of inheritance altogether and simply stating “genetic” or “epigenetic”.
Hi, passionlessdrone. I think I’ll let Robert handle your questions, as I know I don’t have enough background yet to feel comfortable in attempting to answer them. But I’ll let you know if I find anything useful in the book I ordered. I’ll let ya know!
I hope and expect you will write up a post on your findings and I look forward to it.
Hi Emily;
The 60% conundrum.
I went back and read your article and noticed I had overlooked the results. The JAMA article reported a heritability of 59.2% of the MZ twins.This replicates the most referenced British twn study and Autism IAN’s large twin study that also reported a 60% concordance rate in their large sample of MZ twins. This is the 60% conundrum which I would explain is largely to the difference in concordant rates between monochorionic and dichorionic MZ twins who differ in their prenatal environment. I also looked back at the Hallmayer California Autism Twin Study (CATS).
They also found ‘For strict autism, probandwise concordance for male twins was 0.58 for 40 monozygotic pairs (95% confidence interval [CI], 0.42-0.74) and 0.21 for 31 dizygotic pairs (95% CI, 0.09-0.43); for female twins, the concordance was 0.60 for 7 monozygotic pairs (95% CI, 0.28-0.90) and 0.27 for 10 dizygotic pairs (95% CI, 0.09-0.69)’
http://www.ncbi.nlm.nih.gov/pubmed/21727249
Robert, it’ll definitely be interesting to see in future, as twin studies pay more attention to MC v. DC monozygosity, whether your predictions pan out. I won’t be half surprised if they do. 😉
Here’s one study I bookmarked years ago. It involves personality and cognitive ability in MZ twins disruinguished by chorion type. It does relate to autism traits IMHO
http://www.ncbi.nlm.nih.gov/pubmed/7487842?dopt=Abstract:
Very interesting, thanks, Robert!
@RAJ –
That’s a pretty crazy study! Very nicely done!
Just to tie in to a previous comment by pD regarding placenta function being possible determining risk factor, this is from the document Treating Autism is currently preparing: “There are indications that placental function is one of the factors determining negative neurodevelopmental outcome in congenital infections…”
Kitajima, J., Inoue, H., Ohga, S., et al. (2012) Differential transmission and postnatal outcomes in triplets with intrauterine cytomegalovirus infection. Pediatr Dev Pathol. Mar-Apr;15(2):151-5. doi: 10.2350/11-05-1034-CR.
http://www.ncbi.nlm.nih.gov/pubmed/21985463
even more interesting when interesting when you view this in the context of :
Walker, C.K., Anderson, K.W., Milano, K.M., et al. (2013b) Trophoblast inclusions are significantly increased in the placentas of children in families at risk for autism. Biol Psychiatry. 2013 Aug 1;74(3):204-11. doi: 10.1016/j.biopsych.2013.03.006
and placental inclusions being a well known consequence in all sorts of (animal) prenatal infections…
apologies for typos!
this discussion would be incomplete without my favourite subject thrown in 🙂 http://www.ncbi.nlm.nih.gov/pubmed/21840605 — if anyone is taking bets I’ll put loads on such HERV activity and their polymorphisms being THE ‘heritability’ factor in autism
Interesting that HERVs seem to be more richly expressed in stem and progenitor cells.
HERV-H (the one found by Balestieri group as overexpressed in autism I believe) in embryonic stem cells discussed at length here http://www.retrovirology.com/content/9/1/111
Speaking of (neural) progenitor cells and autism, have you seen this recent paper on autoantibodies (would you say chicken or egg?) http://www.sciencedirect.com/science/article/pii/S038776041300168X
I do wonder whether HERVs are expressed more highly in multipotent cells also, e.g., neural stem cells.
That’s very interesting about the neuron-specific antibodies. I wonder if autoantibodies have been exapted for some uses, in terms of protein regulation, aside from the pathological way in which we view it. I don’t currently have access to the full paper. Can you tell me whether they can any indication of the percentage of kids who exhibits neuron-specific antibodies? I’d be curious how common it was.
“The pattern of bands recognized by autistic sera in lysates of NPCs that had differentiated for 7 days was similar to that in lysates prepared from undifferentiated NPCs” …
“The specific NPC protein epitopes targeted by autoantibodies have not been identified in our study, however, they appear to be expressed in NPCs destined to neuronal lineages, as indicated by the expression of neuronal marker Tuj1, but not the astrocyte marker GFAP, in the cells that showed the most intensive immunoreactivity … sera from children with autism most frequently recognized proteins of the molecular sizes of approximately 210 kDa, 150 kDa, 105 kDa, and 50–55 kDa. Immunoreactivity with the protein band at around 150 kDa was recognized by control sera the most frequently and may represent cross-reactivity of autoantibodies in sera with some commonly expressed epitopes.”
Ah okay. Still wondering about the percentage of kids whose sera was reactive to the neural lineage. I’m guessing it didn’t give anything but p-value, etc.
Table 2.
Serum donors (n) with autoantibodies against proteins expressed by NPCs differentiated for 7 days in culture.
Serum donors Recognized proteins (kD)
∼210 ∼150 ∼105 ∼55
Control (n) 18 4 8 3 2 2 3
Autism (n) 22 13 13 12 15 9 0
last two columns are: Multiple proteins recognized and No proteins recognized – so only 3 of controls (20%) had none, and 0 of ASD. hth
Okay, thanks!
Has any research been done to see if there is increased risk in the children of unaffected siblings of individuals with ASD? As the large population of people with ASD ages, I wonder how many of the unaffected siblings are concerned about their children’s risk for autism.
Elana, although the above study included cousins, it didn’t look at inheritance risk between aunts/uncles and nieces/nephews. And I don’t honestly recall reading any studies that looked at those patterns of inheritance, although maybe Robert Jensen can fill me in here.
But from the familial trends of which we do know, we could probably make a few predictions: 1) in cases of autism which appear to be “simplex” meaning that there are no other identifiable instances of autism or related conditions in the close family, the risk is probably minimal and most of these conditions are probably strongly influenced by single rare mutations in the germline; however, 2) in those families considered “multiplex” it’s likely that risk would be much higher. Not as high as is seen in the siblings of those affected, but I would hazard a guess to say that the percentage average could hover around the 6-8% mark in terms of inheritance, similar to what is seen in the above study between half siblings.
Thanks for the rapid response! I’m intrigued by your guesstimates based on half-siblings. I wonder, though, about the applicability of the heritability stats for the future children of the unaffected siblings. Given the number of adult sibs now considering their future offspring, this topic seems like a great prospective study. Or maybe we need more data on the children of individuals with ASD first…
Yes, this could definitely be a good prospective study, particularly in the aid of family planning. Certainly something to keep in mind. Hopefully such studies aren’t too far off. I for one was happy to see 1st cousins included in the above study. Although I’d also love to start seeing grandparents involved in these genetics studies too. Would probably provide good information on multi-generational patterns of inheritance.