“We took my son on a pilgrimage to the Bronx for an evaluation three months after he had a frightening regression in March. He had been receiving early-intervention services for three months and was improving, and then the light in his eyes began to go out. He stopped looking in my eyes, and when I caught his chin in my hand to look in his face, there was nothing there. He was irritable and spun in circles most of the time, and when he did sit down, he kept pushing the same button on a musical toy over and over and couldn’t be engaged. He didn’t even like his beloved books anymore. My son was gone—there was no spark in his face, no sign of life, just dead eyes.”
~ Amy Leal, Little Boy Lost
The story of Amy’s son is not unfamiliar to us, the idea of a child developing normally or somewhat normally suddenly losing language, social, or motor skills and withdrawing into himself, “the dreaded prison of autos, the root meaning of autism” [1]. It happens before a parent’s eyes, leaving panic, helplessness, and dread in its wake. And what’s even worse is that doctors can’t really explain what’s happening or why it’s happening. There’s no way to get a grasp on what the regression is or how it can be stopped. And so parents are left to trial by error in the hope that something, anything, helps.

What’s especially confusing to most people is the idea that symptoms that arise in early childhood can have roots way back in earlier pregnancy. This confusion has lead to a lot of finger-pointing to different environmental agents, such as vaccination, that may be present around the time of regression. However, as the reader will hopefully see by the end of this blog post, there is a difference between concepts of “cause” and “stimulus”.
One important thing to understand is that autism has a lot in common with epilepsy and this is especially the case with regressive autism, which comprises about 30% of the spectrum [2]. As far back as 1999, we have known that the vast majority of kids with regressive autism (~82%) show abnormal epileptiform activity when measured by magnetoencephalography (MEG) [3]. Epileptiform discharges are the abnormal brain wave activity that often occurs between seizures. Approximately 1/3rd of those on the autism spectrum have a seizure disorder, meanwhile an additional 1/3rd have epileptiform discharges without identifiable seizure activity [4, 5]. On the flip side, those children who experience seizures during infancy or early childhood are also at increased risk for developing autism. According to a longitudinal study performed in Iceland, about 14% of young children with unprovoked seizures were later diagnosed with a form of autism [6]. All but one of those children also had intellectual disability, half of which were profoundly affected. Females were also overrepresented in this group at almost 2-to-1.
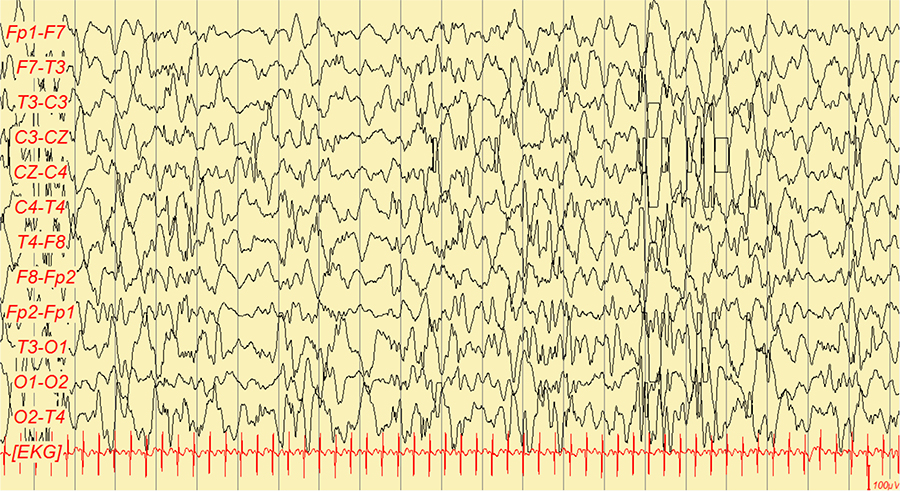
An EEG showing “hypsarrhythmia”, a type of epileptic waveform common to infancy and early childhood periods.
Some forms of seizures are known as “provoked”, meaning that they are brought on by things such as head trauma, low blood sugar, or fever, as opposed to “unprovoked” when there is no discernible cause for the seizure. In particular, fever-induced (febrile) seizures are surprisingly common during the infant and early childhood period [7]. At any given time, approximately 7 in every 1,000 people will have some form of epilepsy, meanwhile 2-5% of infants will experience at least one febrile seizure [8]. Those infants who experience only a single simple febrile seizure typically have low rates of recurrence and recover well; however, infants who have prolonged or complex febrile seizures more often go on to develop full blown epilepsy and may experience other cognitive effects, such as intellectual disability or autism.
Interestingly, some cases of syndromic autism also appear to be “provoked”, and follow similar lines as the seizure progression. Dravet Syndrome, for instance, is a form of infantile epilepsy that also shares a high rate of comorbidity with autism (~25%) and is largely due to mutations in the voltage-gated sodium channel gene, SCN1A [9, 10]. Once seizures start to occur, other symptoms of regression also arise and autistic symptoms may become apparent. Over 2/3rds of those with Dravet Syndrome experience seizures induced by fever [11]. Interestingly, 1/3rd of Dravet infants will experience seizure onset immediately following DPT vaccination, although the timing of onset does not appear to significantly affect these infants’ cognitive outcomes as compared to patients whose seizure onset was not preceded by vaccination [12]. The primary stimulus of seizures appears to be the immune response to either infection or vaccination.
Even though Dravet Syndrome has onset during infancy and may occur following illness or inoculation, there is strong evidence to suggest that its developmental roots lie within the early prenatal period. Le Gal et al. (2010) reported on a child with Dravet Syndrome who was positive for SCN1A mutation. On postmortem study, the researchers found that this child had a type of brain malformation common to epilepsy called a focal cortical dysplasia. Focal cortical dysplasias are strong evidence of early disturbances to the formation of the brain, suggesting that even though seizures don’t occur in Dravet’s until infancy or early childhood, the brain malformations that lead to the condition are formed during pregnancy.
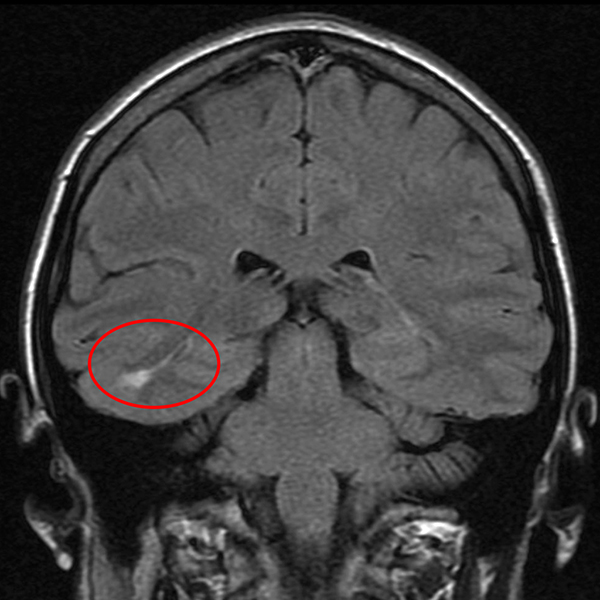
A patient with epilepsy and a focal cortical dysplasia within the temporal lobe. Borrowed from here.
But why do symptoms not become apparent until infancy or later? And why do both epilepsy and autism share this tendency? According to Jensen and Sanchez (2001):
“… the majority of seizures occurring during infancy and early childhood are not spontaneous but are triggered by fever, hypoxia, or trauma. In general, these triggered seizures demonstrate a high degree of age specificity. Hypoxia-related seizures occur primarily in neonates, febrile seizures are exclusive to infancy and childhood, and early traumatic seizures (distinct from posttraumatic epilepsy) are far more common in children” (p. 154).
They go on to suggest that,
“… recent experimental observations from animal models of epilepsy and development suggest that many factors that enhance neuronal excitability are overexpressed during the normal brain maturation. This relative imbalance of excitation over inhibition is postulated to be important for activity-dependent synaptogenesis and synaptic plasticity during a window of development characterized by enhanced rates of learning and brain growth” (p. 154).
So there’s something about the nature of the brain’s excitability during this time period that makes infants more vulnerable to developing a host of related neurological problems, such as epilepsy, autism, and intellectual disability. This is likely why symptoms become most apparent during this time and how a child can suddenly lose numerous skills he’s worked so hard to acquire. It’s not simply because something has happened to him, in reference to illness or vaccination, but because of developmental changes he is going through that are different from the way his brain worked as a young infant and which therefore make him vulnerable.
It’s ironic that the same developmental changes that allow a child to learn and interact with the world are the same changes that risk his withdrawal from it. As with so many of the features that ultimately make us human, there is a cost. In this case, perhaps the evolution of human intelligence has caused us to walk too close to the fire. In the meantime, understanding how these events unfold may help us to eventually treat and perhaps prevent permanent disability in children with this developmental propensity.

I have personally referred a 2 year old with regressive autism for consideration of having Acquired Epileptiform Aphasia (Landau-Kleffner Syndrome). The child was being considered for a diagnosis of autism. The Pediatric Neurologist supported my suspicion and actually diagnosed the child with LKS (AEA). There has been some support for other forms of regressive autism, thinking about the maturation of the brain as a kind of ticking time bomb.
As an aside, I think one of the studies I cited used LKS kids as an additional experimental group. From some of my current genetics studies, this seems to be a common theme amongst different types of genetic epileptic encephalopathies.
Regressive autism is real but is not unique to autism. Schizophrenia origins are almost always in the womb but the severe symptoms do not manifest themselves until decades later.
True, but isn’t it odd that schizophrenia seems to arise in adolescence/adulthood? And those forms that tend to occur in childhood or early adolescence tend to accompany intellectual disability and sometimes autism.
Well, you did mention vaccination, so there is hope….
Charlotte Moore, a Guardian journalist, wrote of her kids childhood. Each time post jab came regression. Clear as could be and all chronicled. Her third boy wasn’t vaccinated. No regressions ever!
I’m still a proponent of vaccination, however I’m also a proponent of doing them smartly. And if there’s cause to suspect a particular child may be vulnerable to unwanted side effects of inoculation, e.g., family history, child’s previous history, etc., then vaccination needs to be seriously reconsidered. The studies on Dravet Syndrome were fascinating, though I disagree with the authors’ recommendations that the vaccination schedule not be altered because there appeared to be no differences in cognitive outcome between those who had a bad reaction and those who didn’t. There should have been further and more thorough investigation to determine whether that was truly the case in all areas of development or whether something was missed by cursory cognitive tests. Also, patterns of regression should be more closely followed, but I think with all this hubbub over vaccination, scientists and doctors are either too stubborn or too scared to give any weight to vaccination concerns. I personally don’t want a society which suddenly stops vaccinating, and in creating panic there’s the possibly large numbers of parents will do so, without reading or listening to the evidence of risk behind the research. I would love to do more research on this topic, however it would be difficult if not impossible to get funded, and I would also worry how the evidence might be misconstrued. But I definitely believe there is need for more research. We have not figured out this story and there are many questions left unanswered.
22q11.2 deletion syndrome is caused by a de novo mutation and many co-occuring medical complications including immune system problems and ASD…
http://www.ncbi.nlm.nih.gov/books/NBK1523/
‘Prevention of secondary complications: Immunization of infants who have lymphocyte abnormalities with live vaccines is not recommended; reevaluate immune status in childhood before giving live vaccines; antibody studies to assess results of immunizations are warranted; irradiated blood products are recommended until normalization of the immune system can be confirmed’.
Excellent to know, Robert. It would be good to put together a listing of these autism-relevant syndromes that are known to be vulnerable to inoculation.
Pingback: Autism Symptoms and Early Signs: What to Look for in Babies … | Early Childhood Parenting·
Pingback: (2005) Autism in Infancy and early childhood – Yale Child Study Center | Early Childhood Parenting·
Pingback: Epidemiology of autism | Early Childhood Parenting·
Pingback: Identifying & Caring for Children with Autism – Earlychildhood NEWS … | Early Childhood Parenting·