In early December, I’ll be giving a grand rounds lecture to clinicians on the topic of coronavirus “long haulers” or “long COVID.” Because the lecture is unfortunately not going to be recorded, I thought it might be helpful to review some of the topics I’ll be covering in the lecture since this is an area of great interest to all, but especially to the chronic illness community.
First off: What is “long COVID” or “long term COVID”? Since the SARS-CoV-2 virus and fallout from its infection are very new to all of us, we’re still in a period of active debate over exactly what is long COVID and how it should be defined. This is despite the fact that the number of papers and media articles on long COVID are increasing by the day. It is very clear that longterm symptoms as a result of coronavirus infection are becoming a major health concern and are affecting a significant subset of people.
At its loosest definition, long COVID refers to any COVID-related symptoms that extend beyond 2-4 weeks following acute symptom onset. Some clinicians and researchers have proposed that long COVID should also be called “postacute COVID” and refer to symptoms that remain between 3-12 weeks after onset of infection. Meanwhile, they have likewise suggested that “chronic post-COVID syndrome” should refer to any symptoms remaining (or developing anew) beyond 12 weeks.
As it stands, however, these are only suggestions. And they still do not take into account the fact that long haulers are a heterogeneous group of people.
Some individuals– particularly those out in the community and not studied in a hospital setting– may experience what is known as a “postviral syndrome”– a range of symptoms, often including chronic fatigue, which are typically seen in other postviral syndromes (e.g., Epstein-Barr virus, herpes, Rubella, etc.). These symptoms are most reminiscent of conditions like myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), mast cell activation syndrome (MCAS), and various dysautonomias like postural orthostatic tachycardia syndrome (POTS).
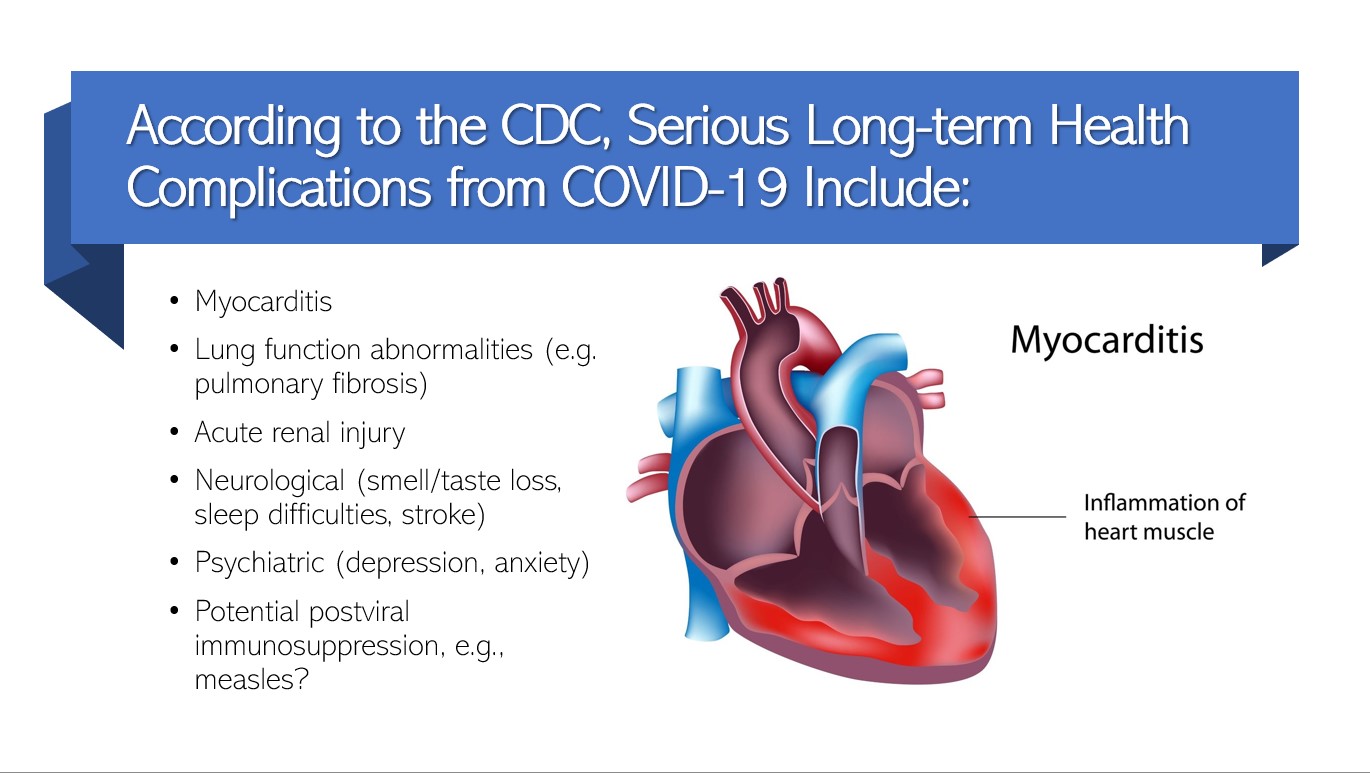
Other people, particularly those who experience severe acute symptoms necessitating hospitalization, are more likely to have chronic illness as a result of organ damage, such as damage to the lungs, heart, or kidneys. This may be either the result of damage due to replication of the virus or because of injury related to treatment, such as ventilation.
Unfortunately, many articles use the term “long hauler” interchangeably for these two groups of people, who may have very different presentations, prognoses, and treatment requirements. So, be wary when reading long hauler articles as to whether they are focusing on patients coming from a hospital setting or out in the community as different subtypes may be overrepresented in these two groups.
Although much of the earlier research into long COVID had focused on patients in hospitals, more recent research has begun to follow COVID sufferers whose acute illness was usually not severe enough to require hospitalization. For the remainder of the article, I’m going to try to focus more on this group of people as they tend to have the most in common with the chronic illness community that I am a part of and which I study.
According to ongoing research, about 10-15% of people develop long COVID. This is very similar to other postviral syndromes (e.g., measles). The most common symptoms of long COVID are:
- Fatigue
- Headache
- Dyspea (shortness of breath)
- Anosmia (loss of smell)
- Pain with deep breaths, chest pain
- Cough
- Joint pain
Other symptoms that are also somewhat common in long COVID include:
- Palpitations
- Tachycardia (rapid heartbeat)
- Concentration and memory issues
- Tinnitus, earache
- Symptoms of peripheral neuropathy (pins and needles, numbness)
- Muscle pain
- Depression
Within long COVID, there are two main patterns or constellations of ongoing symptoms:
- Fatigue, headache, and upper respiratory complaints (shortness of breath, sore throat, persistent cough, loss of smell)
- Ongoing fever and gastrointestinal symptoms
People who experience the following are more likely to experience long COVID:
- Severe illness
- Increasing age
- Higher body mass index (BMI)
- Female sex
- Pre-existing asthma
- Initial symptoms of shortness of breath
- 5 or more symptoms in the first week of infection
In particular, five or more symptoms within the first week are an especially strong predictor of a person going on to develop long COVID.
Like other postviral syndromes, long COVID symptoms are generally episodic, meaning they come and go. For this reason, it is especially important to pace one’s recovery slowly and to be patient with the amount of time it may take to regain previous health. For some individuals, this may mean 6-12 months (or more!) of recovery– a daunting thought for anyone who has not experienced chronic illness before.
Current research suggests that the underlying cause of long COVID involves the innate immune system (especially mast cells) and “cytokine storms” of immune molecules that drive excessive inflammation. There may also be differences in activation of the adaptive immune system (T and B cells) with a shift away from protection against viruses and towards parasites and fungi, for reasons not well understood. This may make it more difficult for the body to clear the virus as efficiently, leading towards an overdependence (and excessive activation) of the innate immune system.
Whatever is ultimately the cause(s) of long COVID, one thing is for certain: It is shining an uncomfortable light on chronic conditions like ME/CFS, MCAS, and POTS, which have typically been ignored by mainstream medicine. Now that we are seeing such large numbers of postviral sufferers in relation to a virus that, at least in some cases, is clinically documented, it makes it extremely difficult for naysayers to continue to deny the links between certain viral infections and chronic illness. Although the numbers of deaths and the toll on overall health and quality of life have been heartbreaking, one silver lining to all of this is the medical community and science can no longer wash away patients’ complaints with a broad psychogenic brush and simply label them as “head cases.”
We must now recognize that these, fundamentally, are immune disorders and they can indeed be triggered by infection.

Thank you so much for making this connection. I have been wondering about this connection to other long-term disease consequences. I have POTS/MCAD/EDS.