I’ve talked a little about heterotopias in the past although I haven’t focused on them considerably. But that’s about to change today because they are fascinating occurrences which happen occasionally within the brain and, if they coincide with some other condition, can often give insight into how the condition developed in the first place. Tuberous Sclerosis is a great example that I’ll touch on later.
What is a heterotopia? This is a term used to describe cells or groups of cells which are migrationally or developmentally misplaced but which still maintain some of the characteristics of the tissue type they were supposed to have been a part of. An excellent example of this is when neurons appear in the white matter tracts of the brain, having failed to migrate properly into the cortex. Frequently, heterotopias are associated with seizure activity, although they also are known to occur in the wider, unaffected general population on occasion without association to any known condition. This is especially true of the nodular type of subcortical heterotopias which will be discussed below.
There are a variety of types of heterotopias that can occur in relation to the neocortex. This may sometimes be individual cells, but more often are seen in larger nodules or full bands of cells or even in ribbon-like arrangements as a semi-separated continuation of the normal cortex. Heterotopias can occur within the subependymal and periventricular (neural stem cell) zone just overlying the ventricles of the brain, and subcortically just beneath the cortical gray matter. The image below is a hemisphere of a normal adult brain to help you visualize where the different heterotopias may occur.

Neuroradiologists tend to divide heterotopias into three main groups, the first two of which can occur either in nodules or larger bands: 1) periventricular/subependymal heterotopias, 2) subcortical heterotopias, and 3) subcortical band heterotopia, as seen in Double Cortex Syndrome. Both periventricular and subcortical forms can occur as either nodular or laminar-like formations, although that has also lead to confusions about the use of “laminar” versus “band” which have been used both interchangeably and distinctly. However, Barkovich and Kjos (1992) state that,
“Radiologically, band heterotopia [as seen in Double Cortex Syndrome] and subcortical heterotopia are distinct. Band heterotopia consist of smooth layers of gray matter that often follow the curvature of the overlying cortex. They are not convoluted nor are they contiguous with the overlying cortex. They do not contain blood vessels or CSF. Subcortical heterotopia usually consist of swirling, heterogeneous, curvilinear masses of gray matter often containing blood vessels and CSF. They are essentially always contiguous with the overlying cortex and the underlying ventricular surface.”
So, basically he suggests that it is better to avoid the use of the term “laminar” altogether, because even though subcortical “laminar” heterotopias may have some sort of laminar or layered appearance, they are less “banded” than the true band heterotopia and do occasionally degrade into a more nodular form. Below is a picture of a subcortical band heterotopia.
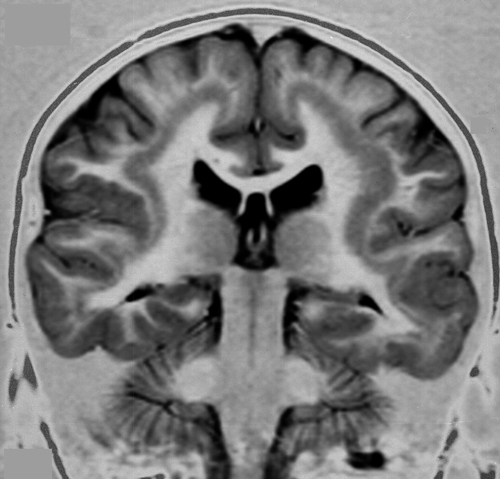
Image of a subcortical band heterotopia, borrowed from here.
Many band heterotopias are thought to be associated with genetic conditions, such as the Double Cortex Syndrome mentioned earlier that is frequently associated with a mutation in the DCX gene. The doublecortin gene interacts with the cytoskeleton of newborn neurons, which has the potential to affect all aspects of cell motility, such as growth and migration. A few cases of Double Cortex Syndrome have also been linked with mutations in LIS1, a protein that interacts with doublecortin. Because the condition is X-linked, females with DCX mutations exhibit the more typical subcortical band heterotopia while males exhibit varying grades of lissencephaly or “smooth brain”.
The well-known autism-associated condition, Tuberous Sclerosis, is also typified by heterotopias, specifically within the periventricular area. Rather than exhibiting focalized heterotopias, people with TSC often have multiple nodular heterotopias, as shown in the image below. Most cases of TSC are due to mutations in the TSC1 and TSC2 genes which are negative regulators of the growth-related Akt pathway. As you can imagine, if one of these genes are knocked out, then activity of Akt increases and subsequently increased cellular growth and proliferation ensues.

Image of periventricular heterotopias, borrowed from here.
So those, folks, are heterotopias. Hopefully you’ve found our little neuropathology class interesting and enlightening. To wrap this up, I’d also like to mention that many people with autism whose brains have been studied postmortem present with heterotopias, particularly nodular forms within the cerebellum and cerebrum. So that really suggests proliferation, differentiation, and perhaps even migration may be altered in the heterogeneous condition. Just some food for thought.

Thank you Emily for covering heterotopias. Those neurons which get a little lost have become my passion and life work after I lost my baby daughter Ella, nearly 5 years ago this upcoming March, when she was just 7 months and 20 days to a then undiagnosed rare disorder. We now know that rare disorder is PVNH4, for short, or X-linked Periventricular Nodular Heteropia with Ehlers-Danlos Syndrome. We also found out at around the same time it span three generations in my family, confirmed with my mom, myself and of course Ella being all affected at various levels. We are one of the rare families without seizures, but with a entire deletion of the FLNA gene which caused Ella’s lungs to be attacked by an interstitial lung disease. As a result, I created an international non-profit organization, PVNH Support & Awareness, which looks after 200+ families in 18 countries at the moment, a few of whom whom also have PVNH4 and whose affected babies required lung resection / double lung transplants for survival. Our mission is to connect families together, advocate and educate patients, family members and medical professionals to positively impact affected individuals’ lives. So thank you for helping me get a little closer to educating the world 🙂 Yolaine
Hi, Yolaine. Thank you very very much for sharing your story. And I’m truly sorry to hear about the loss of your child. That’s heart-wrenching. But I’m glad I can be of a little help in educating the world about heterotopias in the hope we can prevent other suffering. And that’s wonderful that you’ve turned your energies towards helping families like yours. Your dedication is inspiring. I really should make a point of highlighting rare conditions every once in awhile on this blog to help teach people about them. My fiance’s grandson also has a very rare disease, an NGLY1 deficiency, and he is very severely disabled. He was the first to be identified with the condition but they’ve since found some others. We really need to shed more light on these rare conditions! Let’s hope they’re always rare but that, at the very least, it doesn’t take so long to identify them and people can be helped sooner.
hey there im sorry to hear about unfortunate events. I am currently right now going through a living hell my partner has PVNH she has suffered seizures from the age of 14 and she is 27 now she has a heart condition called SVT and has had to have her heart repaced stopped and restarted which after a lot research seems like its linked to her heterotopia, its taken 15 years for one doctor to diagnose her this was very frustrating because nobody would believe us about her seizures I had to keep a daily log of her day to day life and videos aswell,, even tho she finally got diagnosed she had been treated very unfairly on the way she also is going through the full blown menopause, all her life she has been through hell and as we speak she is in hospital as we speak has she has gone very retarded and loss nearly all speech mobility and facial normalities, all this has happened in 10 days its absolutely heartbreaking to see someone you love so much change in no time at all she had had year of normal life before this seizure free from her last episodes and was very much enjoying life with our children we have together 2 & 4, beautiful girls they are but they cant understand why there mummys changed so much and to be honest neither can anybody they don’t seem to know what to do to help her verrryyyyyyyyyy frussstttttrraaaaaaaatttttttttiiiiiiiiiinnnnnnnnnnnnnnngggggggggggg!!!!!!!!!!!!!!!!!!! thank you
Adam, that’s so horrible. Does she have a good neurologist on her team treating her now who knows how to deal with PVNH? Also a cardiologist who is familiar with this syndrome? Take care and positive thoughts to your partner and your family.
By the way, it sounds like getting in touch with vangroovymom who posted above ^^^ could be helpful to you, if you don’t already know her.
Dear Adam,
I am so sorry for what your family has been going through. I would like to offer my help. PVNH Support & Awareness has a private support community with 200+ family members worldwide and we work with leaders, specialists and top researchers around the world too. Many of our members are adult affected individuals or partners of those affected, Contact me here: info at PVNHsupport dot com
In the meantime, please continue to advocate for your partner. Surrounding yourself with a medical team (neuro, cardiologist, geneticist, etc.) that know the disorder and is willing to learn from your partner as she will learn from them (or that are willing to learn about PVNH and collaborate with experts to better care for her) is key. Sending you a great big hug!
And than you Emily again for providing a platform for Adam to find help.
Yolaine Dupont, founder & patient navigator,
PNVH Support & Awareness
More than happy to help. 🙂
thank you very much 🙂 finally we do not feel alone dealing with the heteratopia her neurologist is good but doesn’t quite know enough he knows what condition it is but cant go into detail which led me to do the research, her cardiologist is at a specialist hospital but still they have not linked these conditions together, shes had an ablation on her heart 2 years ago which worked temporary , anybody who treats her just cant seam to come up with a conclusion again I have been to the hospital to visit my lovely partner and they cant conclude if shes had astroke or not she has gained a few motor skills back but her left side is unfeelable I feel so sorry for the way she has been told shes lieing many times even by A&E when she had 6 seizures they told her to stop pretending , this is ridiculous if someone actually listened and believed 15 years ago a nice life may of been good for her but we have two beautiful children 🙂 girls..i am getting all the info and research I have found and making a conclusion to present to the specialist all these problems are because of her cortical heteratopia she also has grey matter on her frontal lobe. there is just not enough people that understand these conditions and I will push and push to make it more well known and present posters and a big collection for personal use of neurologists all around the country . I cant stand the thought of this anybody else sharing our experiences,,,, I will play a strong factor in helping this get known along with you and your community I will stop at nothing 🙂 …. my partner is still in hospital again I cant sleep I cant wait till shes home but I have a lot on when shes back as shes struggling to feed herself at the minute she needs full time care and my children to look after tooo and all this is having no money my benefiets have stopped because us oving back together I have a build up of debt to pay and three ridicoluos forms to fill out to get benefiets again…… we fight for who we love we unite and stay strong nothing else matters right now I hope I don’t crumble …. thank you and over the coming weeks I will be informing you of steps ive made I would very much love to be part of your site as I want to represent information to undertrained doctors
It would be great if Yolaine might recommend some doctors to you who could help consult with your partner’s other doctors. The doctor-patient relationship is sometimes a rocky one, and some doctors have been known to not take “learning from the patient” (or family members of the patient in this case) well. I would highly recommend getting in touch with a specialist who could advocate in your position, Adam. Especially since your partner also needs these doctors whom you are hoping to teach– and some doctors can get their egos bruised very easily I’m sad to say. So think carefully about how you want to present this information to them in a way in which they’ll actually listen and therefore be of more help to your partner. Otherwise, if you present information in a way that gets them defensive, they may be of even less help than they have been already. One of the best ways is to get a fellow doctor– somebody who’s a part of that “club”– to say those things for you.
thank you Emily for your advice I would very much apprieciate if Yolaine could help me out here as I have been to the hospital today for things to get a lot more frustrating her neurologist has finished working with that hospital now and she has been appointed a new neurologist who has obviously not had time to review her notes she very much upset my partner by saying I haven’t said you’ve got cortical heteratopia unfortunately I arrived late to speak to ther new neurologist as I have paperwork from dr hajdu her previous neurologist that clearly says the MRI clearly shows grey matter that is cortical heteratopia within the subependymal layer of the body of the right ventrical,, the neurologist has set up a meeting for me and my partners family to talk about whats happening,, I can really feel the frustration caused from famililes as in yolaines foundation which when I have a moment to myself again I will be joining and supporting her cause and working hard with her and others to raise awareness…. Emily I would like to ask how would you present the information to which seems to me a not well spoken neurologist I have the meeting on Monday , I have numerous videos of my partner having seizure I have research I have done in massive amounts any Ideas ?? your forum is helping me stay strong and I really Hope Yolaine can help my cause as she is a massive inspiration and woman that deserves a medal
That’s a tough one, and perhaps Yolaine could be of some help to you on this one. But first off, it might be a good idea if there’s some way that you can be the official advocate for your partner since she’s obviously not in a good state to communicate and advocate for herself. In which case, it would be understood by the hospital that you be present for any meetings with these doctors. You might ask the hospital about this or, more likely, an attorney/solicitor. If that had been the case with her meeting with the new neurologist, then you would have been there to correct the neurologist and point him to the necessary information so that he’s actually working with the correct diagnosis. (Truthfully, that’s very concerning that he’s not even got the correct diagnosis. If that doesn’t change, I would seriously consider requesting a new neurologist. I’m sure all their staff are very busy, but not having the right diagnosis could be very dangerous should he prescribe treatment for her based on that.)
Next thing is I would start looking for a neurologist who can work with her outpatient. Granted, while she’s in the hospital that won’t be his territory; however, if you can find somebody who has some experience with subcortical heterotopias, that would be ideal. Just prepare the way for when she’s released from the hospital and she can be in more able medical hands.
Last thing, I would really recommend emailing Yolaine right now. I believe she provided her email to you above. See what resources she has to offer you. Support is wonderful, but right now you’re in crisis mode and needing more than just a shoulder. You’re needing practical advice, things you can actually apply, which I’m afraid I’m limited on. So do definitely contact her.
Hospital’s are “interesting” places. And one of your jobs as her partner is not only to help support her and get her better, but to also advocate for her and, if necessary, protect her from any harm that may come from medical negligence. So be calm, civil, but assertive. That’s my best advice.
Hi Adam,
I am Emily’s fiancé. She asked me to read over our comments and provide some thoughts. Seizures are very commonly seen with periventricular nodular heterotopias. Unfortunately they are often multifocal an treatment refractory. Given that she is zoned out, almost unresponsive, and exhibits some left sided weakness, my first guess would have been that she is actively suffering from seizures and her state may be a postictal manifestation. You can read more about this phenomenon from: http://en.wikipedia.org/wiki/Postictal_state. More than anything your partner needs to be evaluated at a neurology unit that specializes in seizures. She may need a 24 hour EEG recording. Regardless of the results, I would treat her as having seizures. If medications do not work or if she suffers side effects from the same, I would investigate the possibility of a ketogenic diet (seehttp://en.wikipedia.org/wiki/Ketogenic_diet). I would also consider seeking help from a geneticist. Periventricular heterotopias are often associated to many genetic conditions. Tuberous sclerosis, for example, has periventricular nodularheterotopias and herat symptoms (including SVT).
I hope that she gets better.
Manuel
Hi I’m new to all this. I’ve a 10 yr old daughter who has complex needs. I’m fighting for 6yrs for help for her but as usual, the parents are blamed, do a parenting course etc. In Sept. 2014 Sarah was diagnosed with Aspergers, ODD (Oppositional Defiant Disorder), sensory issues & mild ADHD. She was diagnosed with mild absence seizures in 2012 & its controlled with meds. Because of Sarah’s aggression (mainly towards me & her 8yr old brother), I asked her neurologist for an MRI (this wasn’t easy as she didn’t see the point in MRI). Bilateral periventricular grey matter heterotopia showed up in scan. At the time the neurologist was shocked over these findings and promised me she would contact Crumlin Hospital in Dublin. But nearly 3yrs later, she seems to have changed her opinion – telling me it’s only a tiny bit in Sarah’s brain & that “we could all have frontal lobe damage but it wouldn’t be confirmed unless we all had MRI” Since Sarah’s violence/aggression has escalated dramatically (I recently ended up in hospital with a damaged wrist – torn liagments, soft tissue & tendons damage), we went to another psychologist. She was the 1st person to tell us – “it’s not Sarah’s autism that is the main cause for her aggression – its the Brain Damage”. Our neurologist does not agree with this, so my GP is now sending in a referral for a 2nd opinion. A Prof. Mary King Paedriatic Neurologist in Temple St, Dublin. Any advice please ?? I feel so helpless and lost & feel like I’ve wasted the last yr or 2 getting help for the ASD when it should have been the grey matter. I’m so disappointed in our current neurologist. Sorry about long post.
Hi, Tanya. Sorry for the delayed reply! I’m actually going to hand my response over to my husband, who is trained in neurology and neuropathology and has far more expertise in this area than I do. So he will be responding shortly. Best of luck!
Thanks Emily, I really appreciate it – there is very little information in Ireland about Frontal Lobe damage – all blaming ASD! Went to GP on Friday and he recommended getting a 2nd opinion – a Prof. Mary King Paedriatric Neurologist in Dublin. But to be honest, I’m nervous that she will say the same thing ie that her Frontal Lobe damage has nothing to do with her violence / aggression. Thanks again Tanya
As an aside, Tanya, while it’s not impossible for someone who’s “normal” to have heterotopias, it’s highly unusual. It’s also not extremely uncommon for people with an autism spectrum condition to have heterotopias. So the heterotopia your daughter has is likely a reflection of the developmental disturbances that have caused her Asperger’s, though the heterotopia itself can cause other issues like seizures and isn’t itself a cause of autism. Think of it more like another symptom of autism, if that makes sense. Here’s an article that you may find interesting, even though it may have a lot of terminology you’re unfamiliar with. In short, it’s a postmortem (after death) series looking at the brains of those with autism and finding, amongst other types of malformations, heterotopias. Table 2 may interest you. http://link.springer.com/article/10.1007/s00401-010-0655-4 –As far as the doc’s opinion that a heterotopia is “no big deal,” I’d definitely find a new doc. That guy sounds like an idiot. Your daughter has multiple developmental disorders and a history of epilepsy and he thinks a heterotopia is an incidental finding? Nope, get a new doc. Listen to your GP. If you find a neurologist who has experience with brain malformations and epilepsies, I doubt they’ll be as dismissive of your concern. Good luck!
Hi Tanya,
Sorry to hear about your problems. Some possibilities come to mind that may be well worth pursuing. Some epileptics may suffer personality changes in-between seizures that may include aggressive behaviors. These behaviors may be more prominent/severe in individuals with a deficiency of executive functions, which your daughter may have because of her autism. Although such an entity may be arguable, it may be worthwhile to examine her behaviors in a hospital setting while being followed with an EEG. Another possibility may be an oppositional defiant disorder that can be seen in children and teens. This condition is more commonly seen in patients with ADHD due to their impulse control problems.I would seriously consider a referral to both a Neurologist and a Child Psychiatrist.
Best regards,
Manuel